Abstract
Among active component service members in 2018, there were 545 incident diagnoses of rhabdomyolysis likely due to exertional rhabdomyolysis, for an unadjusted incidence rate of 42.0 cases per 100,000 person-years. Subgroup-specific rates in 2018 were highest among males, those less than 20 years old, Asian/Pacific Islander service members, Marine Corps and Army members, and those in combat-specific or “other/unknown” occupations. During 2014–2018, crude rates of exertional rhabdomyolysis increased steadily from 2014 through 2016 after which rates declined slightly in 2017 before increasing again in 2018. Compared to service members in other race/ethnicity groups, the overall rate of exertional rhabdomyolysis was highest among non-Hispanic blacks in every year except 2018. Overall and annual rates were highest among Marine Corps members, intermediate among those in the Army, and lowest among those in the Air Force and Navy. Most cases of exertional rhabdomyolysis were diagnosed at installations that support basic combat/recruit training or major ground combat units of the Army or the Marine Corps. Medical care providers should consider exertional rhabdomyolysis in the differential diagnosis when service members (particularly recruits) present with muscular pain or swelling, limited range of motion, or the excretion of dark urine (possibly due to myoglobinuria) after strenuous physical activity, particularly in hot, humid weather.
What Are the New Findings?
The annual numbers and rates of diagnoses of exertional rhabdomyolysis among active component U.S. military members during the 2014–2018 period peaked in 2018. In 2018, for the first time, the annual rate of exertional rhabdomyolysis among Asian/Pacific Islanders was higher than the rate in any other race/ethnicity group.
What Is the Impact on Readiness and Force Health Protection?
The net increase in annual rates of exertional rhabdomyolysis suggests that Commanders, supervisors, and trainers at recruit training camps and at installations with large ground combat units need to be more aggressive in preventing cases of this and other types of heat injury and in detecting early signs of such serious heat-associated injuries.
Background
Rhabdomyolysis is characterized by the breakdown of skeletal muscle cells and the subsequent release of intracellular muscle contents into the circulation. The characteristic triad of rhabdomyolysis includes weakness, myalgias, and red to brown urine (due to myoglobinuria) accompanied by an elevated serum concentration of creatine kinase.1,2 In exertional rhabdomyolysis, damage to skeletal muscle is generally caused by high-intensity, protracted, or repetitive physical activity, usually after engaging in unaccustomed strenuous exercise (especially with eccentric and/or muscle-lengthening contractions).3 Even athletes who are used to intense training and who are being carefully monitored are at risk of this condition,4 especially if new overexertion-inducing exercises are being introduced.5 Illness severity ranges from elevated serum muscle enzyme levels without clinical symptoms to life-threatening disease associated with extreme enzyme elevations, electrolyte imbalances, and kidney failure.1–3,6
Risk factors for exertional rhabdomyolysis include younger age, male sex, a lower level of physical fitness, a prior heat illness, a lower level of education, and exertion during the warmer months of the year.1,3,7–10 Acute kidney injury, due to an excessive concentration of free myoglobin in the urine accompanied by volume depletion, renal tubular obstruction, and renal ischemia, represents a serious complication of rhabdomyolysis.6,11 Severly affected patients can also develop compartment syndrome, fever, dysrhythmias, metabolic acidosis, and altered mental status.
In U.S. military members, rhabdomyolysis is a significant threat during physical exertion, particularly under heat stress.7,9,12–14 Moreover, although rhabdomyolysis can affect any service member, new recruits, who are not yet accustomed to the physical exertion required of basic training, may be at particular risk.9 Each year, the MSMR summarizes the numbers, rates, trends, risk factors, and locations of occurrences of exertional heat injuries, including exertional rhabdomyolysis. This report includes the data for 2014–2018. Additional information about the definition, causes, and prevention of exertional rhabdomyolysis can be found in previous issues of the MSMR.12,13,15
Methods
The surveillance period was 1 Jan. 2014 through 31 Dec. 2018. The surveillance population included all individuals who served in the active component of the Army, Navy, Air Force, or Marine Corps at any time during the surveillance period. All data used to determine incident exertional rhabdomyolysis diagnoses were derived from records routinely maintained in the Defense Medical Surveillance System (DMSS). These records document both ambulatory encounters and hospitalizations of active component members of the U.S. Armed Forces in fixed military and civilian (if reimbursed through the Military Health System [MHS]) treatment facilities worldwide. In-theater diagnoses of exertional rhabdomyolysis were identified from medical records of service members deployed to Southwest Asia/Middle East and whose health care encounters were documented in the Theater Medical Data Store (TMDS).
For this analysis, a case of exertional rhabdomyolysis was defined as an individual with 1) a hospitalization or outpatient medical encounter with a diagnosis in any position of either "rhabdomyolysis" (International Classification of Diseases, 9th Revision [ICD-9]: 728.88; International Classification of Diseases, 10th Revision [ICD-10]: M62.82) or "myoglobinuria" (ICD-9: 791.3; ICD-10: R82.1) plus a diagnosis in any position of 1 of the following: "volume depletion (dehydration)" (ICD-9: 276.5*; ICD-10: E86.0, E86.1, E86.9), "effects of heat" (ICD-9: 992.0–992.9; ICD-10: T67.0–T67.9), {effects of thirst (deprivation of water)" (ICD-9: 994.3; ICD-10: T73.1), "exhaustion due to exposure" (ICD-9: 994.4; ICD-10: T73.2), or "exhaustion due to excessive exertion (overexertion)" (ICD-9: 994.5; ICD-10: T73.3).13 Each individual could be considered an incident case of exertional rhabdomyolysis only once per calendar year.
To exclude cases of rhabdomyolysis that were secondary to traumatic injuries, intoxications, or adverse drug reactions, medical encounters with diagnoses in any position of "injury, poisoning, toxic effects" (ICD-9: 800–999; ICD-10: S00–T88, except the codes specific for "sprains and strains of joints and adjacent muscles" and "effects of heat, thirst, and exhaustion") were not considered indicative of exertional rhabdomyolysis.13
For surveillance purposes, a "recruit trainee" was defined as an active component member in an enlisted grade (E1–E4) who was assigned to 1 of the services’ recruit training locations (per the individual's initial military personnel record). For this report, each service member was considered a recruit trainee for the period of time corresponding to the usual length of recruit training in his or her service. Recruit trainees were considered a separate category of enlisted service members in summaries of rhabdomyolysis cases by military grade overall.
In-theater diagnoses of exertional rhabdomyolysis were analyzed separately; however, the same case-defining criteria and incidence rules were applied to identify incident cases. Records of medical evacuations from the U.S. Central Command (CENTCOM) area of responsibility (AOR) (e.g., Iraq and Afghanistan) to a medical treatment facility outside the CENTCOM AOR also were analyzed separately. Evacuations were considered case defining if affected service members met the above criteria in a permanent military medical facility in the U.S. or Europe from 5 days before to 10 days after their evacuation dates.
The new electronic health record for the MHS, MHS GENESIS, was implemented at several military treatment facilities during 2017. Medical data from sites that are using MHS GENESIS are not available in the DMSS. These sites include Naval Hospital Oak Harbor, Naval Hospital Bremerton, Air Force Medical Services Fairchild, and Madigan Army Medical Center. Therefore, medical encounters for individuals seeking care at any of these facilities during 2017–2018 were not included in this analysis.
Results
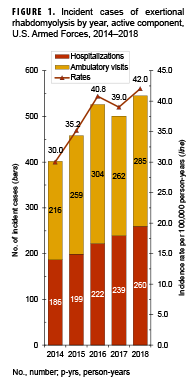
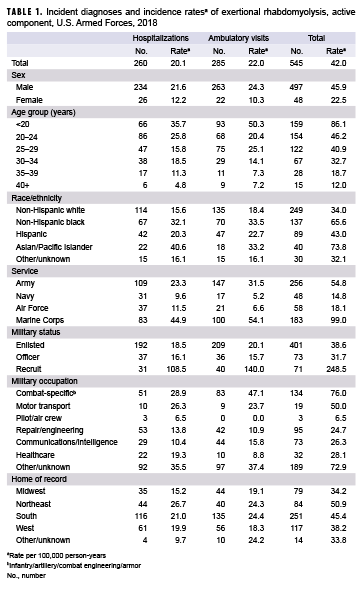
In 2018, there were 545 incident diagnoses of rhabdomyolysis likely associated with physical exertion and/or heat stress (exertional rhabdomyolysis) (Table 1). The crude (unadjusted) incidence rate was 42.0 cases per 100,000 person-years (p-yrs). Subgroup-specific incidence rates of exertional rhabdomyolysis diagnoses were highest among males (45.9 per 100,000 p-yrs), those less than 20 years old (86.1 per 100,000 p-yrs), Asian/Pacific Islander service members (73.8 per 100,000 p-yrs), Marine Corps and Army members (99.0 per 100,000 p-yrs and 54.8 per 100,000 p-yrs, respectively), and those in combat-specific or "other/unknown
occupations (76.0 per 100,000 p-yrs and 72.9 per 100,000 p-yrs, respectively) (Table 1). Of note, the incidence rate among recruit trainees was more than 6 times that among other enlisted members and officers, even though cases among this group accounted for only 13.0% of all cases in 2018.
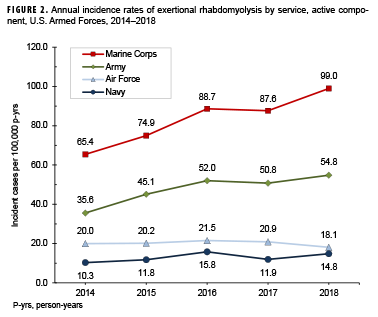
During the surveillance period, crude annual rates of incident diagnoses of exertional rhabdomyolysis increased steadily from 30.0 per 100,000 p-yrs in 2014 to 40.8 per 100,000 p-yrs in 2016 after which rates declined slightly to 39.0 per 100,000 p-yrs in 2017 before increasing again to 42.0 per 100,000 p-yrs in 2018 (Figure 1). During 2014–2018, the annual incidence rates of exertional rhabdomyolysis diagnoses were highest among non-Hispanic blacks in every year except 2018, when the highest rate occurred among Asian/Pacific Islanders (data not shown). Overall and annual rates of incident exertional rhabdomyolysis diagnoses were highest among service members in the Marine Corps, intermediate among those in the Army, and lowest among those in the Air Force and Navy (Table 1, Figure 2). The most pronounced increases in annual incidence rates were observed among Marine Corps members and Army members during 2014–2016 (35.5% and 46.2%, respectively); however, rates among service members in the Air Force and Navy remained relatively stable (Figure 2). During the surveillance period, approximately three-quarters (75.6%) of the cases occurred during May–Oct. (Figure 3).
Rhabdomyolysis by location
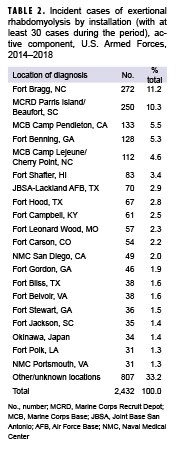
During the 5-year surveillance period, the medical treatment facilities at 11 installations diagnosed at least 50 cases each; when combined, these installations diagnosed almost half (47.7%) of all cases (Table 2). Of these 11 installations, 4 provide support to recruit/basic combat training centers (Marine Corps Recruit Depot Parris Island/Beaufort, SC; Fort Benning, GA; Joint Base San Antonio–Lackland, TX; and Fort Leonard Wood, MO). In addition, 6 installations support large combat troop populations (Fort Bragg, NC; Marine Corps Base [MCB] Camp Pendleton, CA; MCB Camp Lejeune/Cherry Point, NC; Fort Shafter, HI; Fort Hood, TX; and Fort Campbell, KY). The most cases overall were diagnosed at Fort Bragg, NC (n=272) and MCRD Parris Island/Beaufort, SC (n=250), which together accounted for more than one-fifth (22.5%) of all cases (Table 2).
Rhabdomyolysis in Iraq and Afghanistan
There were 6 incident cases of exertional rhabdomyolysis diagnosed and treated in Iraq/Afghanistan (data not shown) during the 5-year surveillance period. Deployed service members who were affected by exertional rhabdomyolysis were more often non-Hispanic black or non-Hispanic white (n=4; 66.7% and n=2; 33.3%, respectively), male (n=6), aged 20–24 years (n=2; 33.3%), in the Army (n=6), enlisted (n=6), and in communication/intelligence occupations (n=2; 33.3%). One active component service member was medically evacuated from Iraq/Afghanistan for exertional rhabdomyolysis; this medical evacuation occurred in Sept. 2015 (data not shown).
Editorial Comment
This report documents an increase in the crude annual incidence rates of diagnoses of exertional rhabdomyolysis among active component U.S. military members from 2014 through 2016 after which rates declined slightly in 2017 before increasing again in 2018. Exertional rhabdomyolysis continued to occur most frequently from late spring through early fall at installations that support basic combat/recruit training or major Army or Marine Corps combat units.
The risks of heat injuries, including exertional rhabdomyolysis, are increased among individuals who suddenly increase overall levels of physical activity, recruits who are not physically fit when they begin training, and recruits from relatively cool and dry climates who may not be acclimated to the high heat and humidity at training camps in the summer.1,2,9 Soldiers and Marines in combat units often conduct rigorous unit physical training, personal fitness training, and field training exercises regardless of weather conditions. Thus, it is not surprising that recruit camps and installations with large ground combat units account for most of the cases of exertional rhabdomyolysis.
The annual incidence rates among non-Hispanic black service members were higher than the rates among members of other race/ethnicity groups in 4 of the 5 previous years, with the exception of 2018. This observation has been attributed, at least in part, to an increased risk of exertional rhabdomyolysis among individuals with sickle cell trait16–19 and is supported by at least 1 other study among U.S. service members.9 However, in 2018, the rate among Asian/Pacific Islanders was the highest of all race/ethnicity groups. Although the annual incidence rates of exertional rhabdomyolysis for service members in this group have been increasing since 2009, the reasons for such a trend are unknown. Supervisors at all levels should ensure that guidelines to prevent heat injuries are consistently implemented and should be vigilant for early signs of exertional heat injuries, including rhabdomyolysis, among all service members.
The findings of this report should be interpreted with consideration of its limitations. A diagnosis of "rhabdomyolysis" alone does not indicate the cause. Ascertainment of the probable causes of cases of exertional rhabdomyolysis was attempted by using a combination of ICD-9/ICD-10 diagnostic codes related to rhabdomyolysis with additional codes indicative of the effects of exertion, heat, or dehydration. Furthermore, other ICD-9/ICD-10 codes were used to exclude cases of rhabdomyolysis that may have been secondary to trauma, intoxication, or adverse drug reactions.
The measures that are effective at preventing exertional heat injuries in general apply to the prevention of exertional rhabdomyolysis. In the military training setting, the risk of exertional rhabdomyolysis can be reduced by emphasizing graded, individual preconditioning before starting a more strenuous exercise program and by adhering to recommended work/rest and hydration schedules, especially in hot weather. The physical activities of overweight and/or previously sedentary new recruits should be closely monitored. Strenuous activities during relatively cool mornings following days of high heat stress should be particularly closely monitored; in the past, such situations have been associated with increased risk of exertional heat injuries (including rhabdomyolysis).8
Management after treatment for exertional rhabdomyolysis, including the decision to return to physical activity and duty, is a persistent challenge among athletes and military members.9,10,20 It is recommended that those who have had a clinically confirmed exertional rhabdomyolysis event be further evaluated and risk stratified for recurrence before return to activity/duty.10,21,22 Low-risk patients may gradually return to normal activity levels, while those deemed high risk for recurrence will require further evaluative testing (e.g., genetic testing for myopathic disorders).20,21
Commanders and supervisors at all levels should watch for early signs of exertional heat injuries and should intervene aggressively when dangerous conditions, activities, or suspicious illnesses are detected. Finally, medical care providers should consider exertional rhabdomyolysis in the differential diagnosis when service members (particularly recruits) present with muscular pain or swelling, limited range of motion, or the excretion of dark urine (possibly due to myoglobinuria) after strenuous physical activity, particularly in hot, humid weather.
References
- Zutt R, van der Kooi AJ, Linthorst GE, Wanders RJ, de Visser M. Rhabdomyolysis: review of the literature. Neuromuscul Disord. 2014;24(8):651–659.
- Giannoglou GD, Chatzizisis YS, Misirli G. The syndrome of rhabdomyolysis: pathophysiology and diagnosis. Eur J Intern Med. 2007;18(2):90–100.
- Rawson ES, Clarkson PM, Tarnopolsky MA. Perspectives on exertional rhabdomyolysis. Sports Med. 2017;47(Suppl 1):33–49.
- McKewon S. Two Nebraska football players hospitalized, treated after offseason workout.Omaha World-Herald. 20 Jan. 2019. https://www.omaha.com/huskers/football/two-nebraskafootball-players-hospitalized-treated-after-offseason-workout/article_d5929674-53a7-5d90-803e-6b4e9205ee60.html. Accessed 06 March 2019.
- Raleigh MF, Barrett JP, Jones BD, Beutler AI, Deuster PA, O'Connor FG. A cluster of exertional rhabdomyolysis cases in a ROTC program engaged in an extreme exercise program. Mil Med. 2018;183(suppl 1):516–521.
- Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009;361(1):62–72.
- Hill OT, Wahi MM, Carter R, Kay AB, McKinnon CJ, Wallace RE. Rhabdomyolysis in the U.S. active duty Army, 2004–2006. Med Sci Sports Exerc. 2012;44(3):442–449.
- Lee G. Exercise-induced rhabdomyolysis. R I Med J (2013). 2014;97(11):22–24.
- Hill OT, Scofield DE, Usedom J, et al. Risk factors for rhabdomyolysis in the U.S. Army. Mil Med. 2017;182(7):e1836–e1841.
- Knapik JJ, O'Connor FG. Exertional rhabdomyolysis: epidemiology, diagnosis, treatment, and prevention. J Spec Oper Med. 2016;15(3):65–71.
- Holt S, Moore K. Pathogenesis of renal failure in rhabdomyolysis: the role of myoglobin. Exp Nephrol. 2000;8(2):72–76.
- Armed Forces Health Surveillance Branch. Update: Exertional rhabdomyolysis, active component, U.S. Army, Navy, Air Force, and Marine Corps, 2011–2015. MSMR. 2016;23(3):21–24.
- Armed Forces Health Surveillance Branch. Update: Exertional rhabdomyolysis among active component members, U.S. Armed Forces, 2012–2016. MSMR. 2017;24(3):14–18.
- Armed Forces Health Surveillance Branch. Update: Exertional rhabdomyolysis among active component members, U.S. Armed Forces, 2013–2017. MSMR. 2018;25(4):13–17.
- Armed Forces Health Surveillance Branch. Surveillance Case Definition. Exertional Rhabdomyolysis. April 2017. https://www.health.mil/Reference-Center/Publications/2017/03/01/Rhabdomyolysis-Exertional. Accessed 05 March 2019.
- Gardner JW, Kark JA. Fatal rhabdomyolysis presenting as mild heat illness in military training. Mil Med. 1994;159(2):160–163.
- Makaryus JN, Catanzaro JN, Katona KC. Exrtional rhabdomyolysis and renal failure in patients with sickle cell trait: is it time to change our approach? Hematology. 2007;12(4):349–352.
- Ferster K, Eichner ER. Exertional sickling deaths in Army recruits with sickle cell trait. Mil Med. 2012;177(1):56–59.
- Nelson DA, Deuster PA, Kurina LM. Sickle cell trait and rhabdomyolysis among U.S. Army soldiers. N Engl J Med. 2016;375(17):1696.
- O’Connor FG, Brennan FH Jr, Campbell W, Heled Y, Deuster P. Return to physical activity after exertional rhabdomyolysis. Curr Sports Med Rep. 2008;7(6):328–331.
- Atias D, Druyan A, Heled Y. Recurrent exertional rhabdomyolysis: coincidence, syndrome, or acquired myopathy? Curr Sports Med Rep. 2013;12(6):365–369.