The most serious types of heat illness, heat exhaustion and heat stroke, are occupational hazards of the military’s training and operational environments. These conditions can be mitigated with appropriate situational awareness and effective countermeasures. In 2022, the crude incidence rates of heat stroke and heat exhaustion among active component service members were 32.1 and 147.7 per 100,000 person-years, respectively. The rates of incident heat stroke and heat exhaustion generally declined during the 2018 to 2022 surveillance period. In 2022, those at highest risk were men, those younger than age 20, Marine Corps and Army members, recruit trainees, and those in combat-specific occupations. Leaders, training cadres, and supporting medical personnel must inform their supervised and supported service members of heat illness risks, preventive measures, early signs and symptoms, and first-responder actions.
What are the new findings?
The crude annual incidence rates of heat stroke and heat exhaustion decreased 30.0% and 15.1%, respectively, from 2018 to 2022. The annual number of heat illnesses diagnosed in the CENTCOM AOR dropped from a high of 73 in 2019 to 48 in 2022, likely due to the reduction in forces deployed there. Only about half of heat stroke and heat exhaustion cases were identified in mandatory reports submitted to the Disease Reporting System internet.
What is the impact on readiness and force health protection?
Heat illness can be fatal, even with prompt recognition and treatment. Situational awareness and implementation and enforcement of appropriate countermeasures by commanders at all levels are the most effective means of reducing incidence of these preventable illnesses. Complete, timely submission of mandatory reports of heat illness events ensures that local public health and command leaders have ready access to surveillance data, to identify trends and guide preventive measures.
Background
Heat-related illness remains a persistent threat to the health and operational effectiveness of military members and their units, and accounts for considerable annual morbidity. Strenuous physical activity for extended durations during operational and training exercises exposes service members to considerable heat stress due to the absorption of high environmental heat along with elevated rates of metabolic heat production.1,2 Although numerous effective countermeasures are available, operational necessity may preclude their full employment. Deconditioned and unacclimated service members are at particularly high risk, as exemplified by the rates of heat injuries during U.S. military recruit training.1,3-5
Heat illness refers to a group of disorders that result from core body temperature surpassing the compensatory limits of thermoregulation6 due to environmental heat stress, usually accompanied by heavy exertion. Heat illness constitutes a set of conditions along a continuum, from less severe (heat cramps, rash, edema, and syncope) to potentially life-threatening (heat stroke). The DOD definition of reportable heat illness includes only heat exhaustion and heat stroke, the 2 conditions covered in this report. Heat exhaustion and heat stroke are reportable medical events (RMEs) in the U.S. Military Health System (MHS), and all cases of heat illness that require medical intervention or result in change of duty status are reportable.7
To be confirmed, a case of heat exhaustion must fulfill 3 conditions, during or immediately following exertion or heat exposure: 1) a core body temperature greater than 100.5º F / 38º C and less than 104º F / 40º C, 2) short-term physical collapse or debilitation during or shortly after physical exertion, and 3) no significant central nervous system dysfunction.5 Acute dehydration often accompanies heat exhaustion but is not required for diagnosis.8 If any central nervous system dysfunction develops (e.g., dizziness or headache), it should be mild and rapidly resolve with rest and cooling measures.5,8
Heat stroke is a debilitating and potentially life-threatening condition characterized by severe hyperthermia. A probable case of heat stroke requires, concomitant to the setting of exertion or heat exposure, 1) evidence of elevated core body temperature and 2) central nervous system dysfunction (change in mental status, delirium, stupor, loss of consciousness, or coma). A confirmed case of heat stroke requires verification and documentation of a core body temperature of 104º F / 40º C or greater with central nervous system dysfunction.8,9 The onset of heat stroke should prompt aggressive clinical treatment featuring rapid cooling and supportive therapy such as fluid resuscitation to stabilize organ function.8-10 Multiorgan system failure is the ultimate cause of mortality from heat stroke.9
Heat illnesses represent a threat to the health of individual service members during military training and operations, but are frequently preventable. Mitigation methods include heat acclimatization, sufficient hydration, mandated work-rest cycles, uniform modifications to improve evaporative heat loss, limiting weight loads during training, and scheduling high intensity exercise during cooler times of day.3,11-14
Since 2001, the MSMR has published regular updates on the incidence of heat illness among U.S. active duty service members. This report presents the case counts and incidence rates of heat illnesses between 2018 and 2022 as well as the locations of heat illness case occurrences during this period. Heat stroke and heat exhaustion are summarized separately.
Methods
The surveillance population for this analysis includes all individuals who served in the active component of the Army, Navy, Air Force, or Marine Corps at any time during the surveillance period of January 1, 2018 through December 31, 2022. All data used to determine incident heat illness diagnoses were derived from records routinely maintained in the Defense Medical Surveillance System (DMSS), which documents both ambulatory care encounters and hospitalizations of active component service members of the U.S. Armed Forces in fixed military and civilian (if reimbursed through MHS) treatment facilities worldwide. In-theater diagnoses of heat illness were identified from medical records of deployed service members whose health care encounters were documented in the Theater Medical Data Store. Because they are an occupational hazard of rigorous outdoor training intrinsic to the military, and often preventable, heat illnesses are RMEs recorded within service-specific electronic reporting systems that are routinely transmitted and incorporated into the DMSS.
In this update, the same definition for heat illness was used as in MSMR reports since 2018. A case of heat illness was defined as an individual with 1) a hospitalization or outpatient medical encounter record with a primary (first-listed) or secondary (second-listed) diagnosis of heat stroke (International Classification of Diseases, 9th Revision [ICD-9]: 992.0; International Classification of Diseases, 10th Revision [ICD-10]: T67.0*) or heat exhaustion (ICD-9: 92.3–992.5; ICD-10: T67.3*–T67.5*) or 2) an RME record of heat exhaustion or heat stroke.15 Because of a July 2017 update to the Disease Reporting System internet (DRSi) medical event reporting system, the type of heat illness (i.e., heat stroke or heat exhaustion) could not be distinguished using RME records in DMSS data. Instead, information on the type of RME for heat illness during the entire 2018-2022 surveillance period was extracted directly from DRSi records. MSMR analyses before 2018 included diagnosis codes for other and unspecified effects of heat and light (ICD-9: 992.8 and 992.9; ICD-10: T67.8* and T67.9*) within an “other heat illnesses” category; these codes were excluded from this report.
An individual could be considered a case of heat illness only once per calendar year. If a service member had a diagnosis for both heat stroke and heat exhaustion during a given year, the more severe (heat stroke) diagnosis was selected. Order of precedence for encounter selection followed: 1) hospitalization (inpatient record), 2) RME (report in DRSi), then 3) ambulatory visit (outpatient record). Incidence rates were calculated as incident cases of heat illness per 100,000 person-years (p-yrs) of active component service. Percent change in incidence was calculated using unrounded rates.
For health surveillance purposes, recruit trainees were identified as active component members assigned to service-specific training locations during coincident service-specific basic training periods. Recruit trainees were considered a separate category of enlisted service members in summaries of heat illnesses by overall military grade.
In-theater diagnoses of heat illnesses were analyzed separately using the same case-defining criteria and incidence rules that were applied to identify cases at fixed treatment facilities. Records of medical evacuations from the U.S. Central Command (CENTCOM) area of responsibility (AOR) to a medical treatment facility outside their AOR were analyzed separately. Evacuations were considered case defining if the affected service members met the aforementioned criteria in a permanent military medical facility in the U.S. or Europe, from 5 days preceding until 10 days following their evacuation dates.
Results
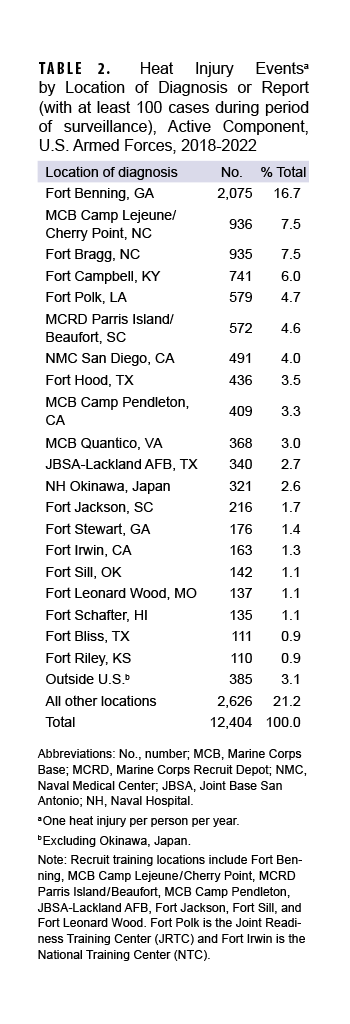
In 2022, the MHS reported 415 cases of heat stroke, resulting in a crude overall incidence rate of 32.1 per 100,000 p-yrs (Table 1).
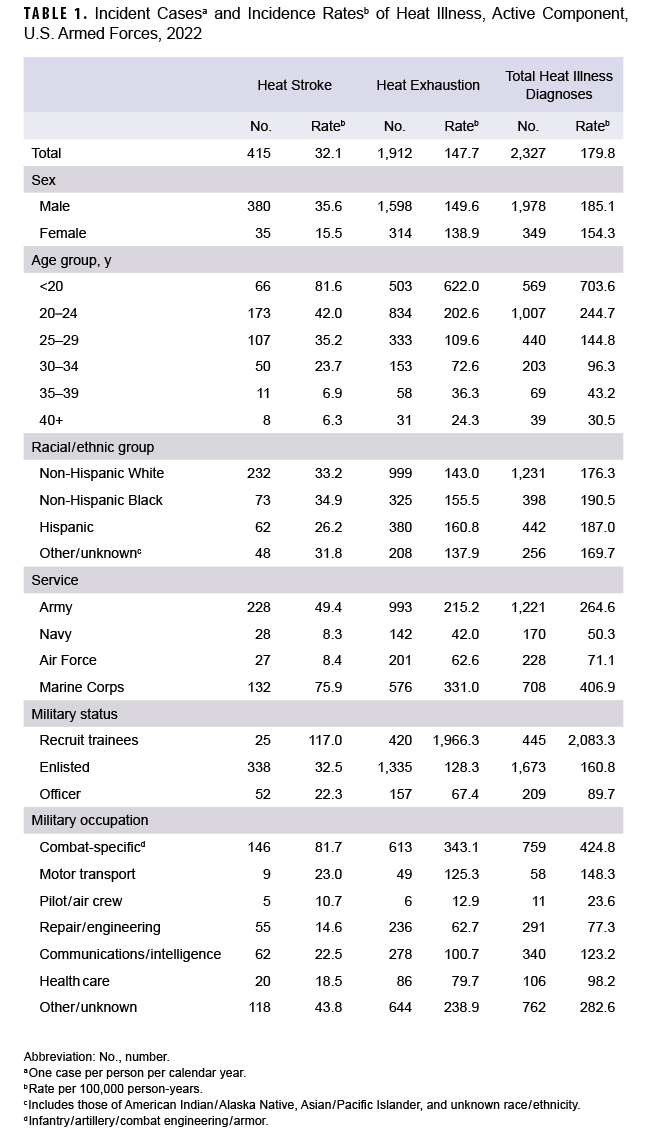
Subgroup-specific incidence rates of heat stroke were highest among men, those younger than 20 years, Marine Corps and Army members, recruit trainees, and those in combat-specific occupations. The 25 cases of heat stroke reported among recruit trainees resulted in incidence rates 3 and 6 times higher than other enlisted service members and officers, respectively.
The crude annual incidence rate of heat stroke decreased 30.0% (Figure 1) from 2018 through 2022, and was associated with an overall reduction in the proportion of heat stroke cases with hospitalization, which dropped most markedly from 2021 to 2022. Of the heat stroke cases identified from inpatient data, 55.7% were also reported as RMEs. Half (50.7%) of cases identified from outpatient data were also recorded as RMEs.
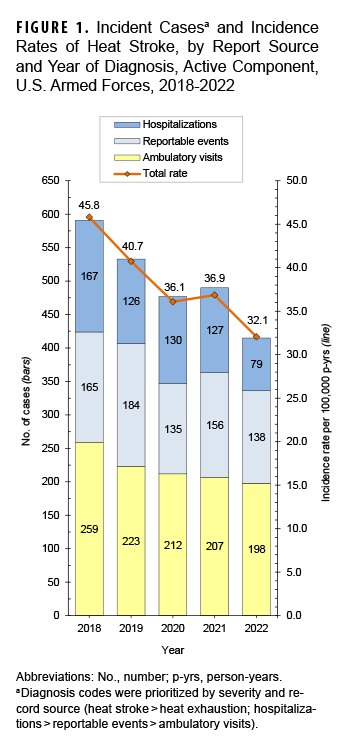
The 1,912 cases of heat exhaustion in 2022 correspond to a crude overall incidence rate of 147.7 per 100,000 p-yrs (Table 1). The rate of heat exhaustion among women was 16.6% lower than the rate among men. Notably higher overall rates of heat exhaustion were recorded for service members younger than age 20, Marine Corps and Army members, recruit trainees, and service members in combat-specific occupations when compared to their respective counterparts.
Between 2018 and 2020, the crude annual rate of heat exhaustion decreased 27.4%, followed by a 16.8% increase from 2020 to 2022 (Figure 2).
The increase in heat exhaustion cases during the last two years of the surveillance period was accompanied by an increase in the proportion of cases recorded as RMEs. Of the heat exhaustion cases identified from inpatient data, 54.5% were also RMEs, while only 39.2% of heat exhaustion cases identified from outpatient data were recorded as RMEs.
Heat illnesses by location
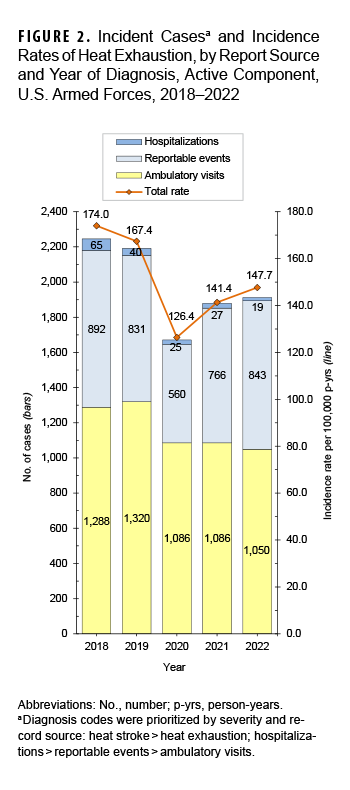
During the 5-year surveillance period, 12,404 heat-related illnesses were diagnosed at more than 250 military installations and geographic locations worldwide (Table 2).
Of these total heat illness cases, 5.7% occurred outside the U.S., including 321 in Okinawa. Between 2018 and 2022, 20 locations reported at least 100 cases of heat illness, and those locations accounted for over three-quarters (75.7%) of all active component cases. Four Army installations in the U.S. accounted for more than one-third (34.9%) of all heat illnesses during the period: Fort Benning, GA; Fort Bragg, NC; Fort Campbell, KY; and Fort Polk, LA. Of the 20 locations with at least 100 cases of heat illness, 9 are in the southeastern U.S.
Heat illnesses in the CENTCOM AOR
During the 5-year surveillance period, 293 heat illnesses were diagnosed and treated in the CENTCOM AOR (Figure 3).
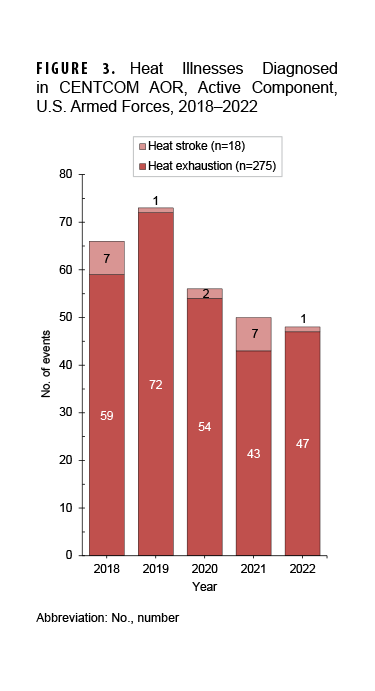
Of the total cases of heat illness, 6.1% (n=18) were diagnosed as heat stroke. Deployed service members affected by heat illnesses were most frequently male (n=225; 76.8%), non-Hispanic White (n=153; 52.2%), 20-24 years old (n=153; 52.2%), in the Army (n=113; 38.6%), enlisted (n=280; 95.6%), and in repair/engineering (n=96; 32.8%) occupations (data not shown). During the surveillance period, 2 service members were medically evacuated for heat illnesses from the CENTCOM AOR; 1 evacuation occurred in November 2020 and 1 in August 2022 (data not shown).
Discussion
Among service members in the active component, the crude incidence rate of heat stroke decreased 30.0% between 2018 and 2022, accompanied by an overall reduction in the proportion of heat stroke cases resulting in hospitalization. While between 2018 and 2020 the rate of heat exhaustion also declined by approximately 30%, rates then increased through 2022. This increase in heat exhaustion cases observed in the last 2 years of the surveillance period coincides with an increase in the proportion of cases identified from RMEs.
As has been noted in previous MSMR heat illness updates, results indicate that a sizable proportion of cases identified through DMSS records (hospitalizations and ambulatory visits) did not prompt mandatory reports through the reporting system.12 In 2022, only about half of heat illness cases were accompanied by RMEs. It is possible that cases of heat illness, whether diagnosed during an inpatient or outpatient encounter, were not documented as RMEs either because treatment providers were unaware of the reporting criteria, or due to ambiguities in their criteria interpretation. Underreporting is especially concerning for cases of heat stroke due to its severity and potential necessity of timely local intervention for preventing additional cases.
In 2022, rates of heat stroke and heat exhaustion were slightly higher among men than women, which is not consistent with published observational studies of military personnel that reported elevated risk of exertional heat illness among women.13 Because this finding may be due to variation in true exposure time rather than physiologic or morphologic differences in body temperature responses between men and women, further investigation is warranted.
Of all members of the military, Marine Corps and Army recruit trainees, particularly those training at installations in the southeastern U.S., along with those in combat-specific occupations, suffered the highest rates of heat stroke and heat exhaustion. Army and Marine Corps members in combat units often engage in intense physical training, field training exercises, as well as personal fitness training in varied environmental conditions, which may account, at least in part, for this finding. The annual numbers of heat illnesses diagnosed in the CENTCOM AOR have declined since 2019, likely due to the reduction in forces deployed to that area.
There are limitations to this update that should be considered when interpreting these results. Because management and coding of similar heat-related clinical illnesses are often location-specific, direct rate comparisons of nominal heat stroke and heat exhaustion events could be imprecise when comparing cases from different locations and settings. Heat illnesses during training exercises and deployments treated in field medical facilities were potentially not fully ascertained as cases for this report. Recruit trainees were identified using an algorithm based on age, rank, location, and time in service. This method was only an approximation and likely resulted in some misclassification of recruit training status. At the time of the analysis, Army personnel data were not available for November and December 2022. Therefore, personnel data were imputed from previous months, which likely resulted in the underestimation of Army recruits and periods of recruit training during the last 2 months of 2022. Due to this data discrepancy, recruit rates should be interpreted with caution.
The guidelines for mandatory heat illness reporting were modified in the 2017 revision of the Armed Forces guidelines and RME case definitions and remained in the 2020 revision.7 This updated version of the guidelines and case definitions removed the heat injury category, leaving only case classifications for heat stroke and heat exhaustion. To compensate for possible reporting variation, the analysis for this update, as in previous years, included cases identified in DMSS records of ambulatory care and hospitalizations using a consistent set of ICD-10 codes for the entire surveillance period. The exclusion of diagnosis codes for other and unspecified effects of heat and light (formerly included within the “other heat illnesses” category) in the current analysis precludes direct comparison of numbers and rates of cases of heat exhaustion to numbers and rates of “other heat illnesses” reported in MSMR updates before 2018. It should be noted that medical data from July 2017 to October 2019 at sites using the new MHS electronic health record, MHS GENESIS, are not available in the DMSS and thus not included in this report——these sites include Naval Hospital Oak Harbor, Naval Hospital Bremerton, Air Force Medical Services Fairchild, and Madigan Army Medical Center.
Heat illnesses, which are largely preventable, remain a persistent threat to both the health of U.S. military members and the effectiveness of military operations. Appropriate command emphasis, recognition, and employment of preventive countermeasures for heat illness are crucial steps in effective risk reduction.
References
- Carter R, Cheuvront SN, Williams JO, et al. Epidemiology of hospitalizations and deaths from heat illness in soldiers. Med Sci Sports Exerc. 2005;37(8):1338-1344. doi:10.1249/01.mss.0000174895.19639.ed
- Hancock PA, Ross JM, Szalma JL. A meta-analysis of performance response under thermal stressors. Hum Factors. 2007;49(5):851-877. doi:10.1518/001872007X230226
-
DeGroot, D., Henderson, K., O’Connor, F. Exertional heat illness at Fort Benning, GA: Unique insights from the Army Heat Center. MSMR.2022;29(4):2-7.
-
Armed Forces Health Surveillance Division. Update: heat illness, active component, U.S. Armed Forces, 2021. MSMR. 2022;29(4):8-14.
-
Alele FO, Bunmi SM, Aduli EOM, Crow MJ. Epidemiology of exertional heat illness in the military: a systematic review of observational studies. Int J Environ Res Public Health. 2020;17(19):7037. doi:10.3390/ijerph17197037
-
Atha WF. Heat-related illness. Emerg Med Clin North Am. 2013;31(4):1097-1108. doi:10.1016/j.emc.2013.07.012
-
Armed Forces Health Surveillance Branch, Defense Health Agency. In collaboration with U.S. Air Force School of Aerospace Medicine, Army Public Health Center, and Navy and Marine Corps Public Health Center. Armed Forces Reportable Medical Events. Guidelines and Case Definitions, January 2020. Accessed March 3, 2022. https://www.med.navy.mil/Portals/62/Documents/NMFA/NMCPHC/root/Documents/program-and-policy-support/Armed-Forces-Reportable-Medical-Events-DOD-VERSION.pdf
-
O’Connor FG, Sawka MN, Deuster P. Disorders due to heat and cold. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 25th ed. Philadelphia, PA: Elsevier Saunders; 2016:692-693.
-
Epstein Y, Yanovich R. Heatstroke. N Engl J Med. 2019;380(25):2449-2459. doi:10.1056/NEJMra1810762
-
DeGroot DW, O’Connor FG, Roberts WO. Exertional heat stroke: an evidence-based approach to clinical assessment and management. Exp Physiol. 2022;107(10):1172-1183. doi:10.1113/EP090488
-
Périard JD, DeGroot D, Jay O. Exertional heatstroke in sport and the military: epidemiology and mitigation. Exp Physiol. 2022;107(10):1111-1121. doi:10.1113/EP090686
-
Headquarters, Department of the Army. Heat Stress Control and Heat Casualty Management Technical Bulletin, Medical, 507. April 12, 2022.
-
Périard JD, Eijsvogels TMH, Daanen HAM. Exercise under heat stress: thermoregulation, hydration, performance implications and mitigation strategies. Physiol Rev. 2021;101(4):1873-1979. doi:10.1152/physrev.00038
-
Roberts WO, Armstrong LE, Sawka MN, Yeargin SW, Heled Y, O’Connor FG. ACSM expert consensus statement on exertional heat illness: recognition, management, and return to activity. Curr Sports Med Rep. 2021;20(9):470-484. doi:10.1249/JSR.0000000000000878
-
Armed Forces Health Surveillance Branch. Surveillance Case Definition: Heat illness. Accessed on March 13, 2022. https://health.mil/Reference-Center/Publications/2019/10/01/Heat-Injuries