Inpatient and outpatient encounter data retrieved from the Defense Medical Surveillance System were used to establish that there were 1,127 diagnoses of systemic lupus erythematosus among active component U.S. service members from 2000 to 2022, with an overall incidence rate of 3.5 cases per 100,000 person-years. Annual incidence remained relatively constant over the 23-year surveillance period, peaking in 2009. Female ACSM accounted for 69.5% of incident cases, with a rate of incidence 12.3 times greater than males, while non-Hispanic Black ACSM accounted for 50.0% of incident cases, with a rate 6.7 times greater than among non-Hispanic Whites. This study further demonstrates greatest SLE incidence among non-Hispanic Black women, in all age groups.
What are the new findings?
SLE incidence among ACSM remained relatively stable from 2000 to 2022. Incidence was notably highest among non-Hispanic Black women in all age groups.
What is the impact on readiness and force health protection?
SLE imposes a substantial burden upon afflicted individuals. Diagnosed ACSM may experience declines in mental and physical acuity that are required for mission execution. Evaluating SLE incidence helps identify factors that contribute to its trends, for early diagnosis and management.
Background
The most common type of lupus is systemic lupus erythematosus, a chronic autoimmune disease that is often difficult to diagnose due to its complex clinical presentations.1,2 This disease imposes a substantial burden for those who develop a myriad of symptoms ranging from fatigue to organ damage.2 The literature on representative, population-based, national U.S. studies of SLE incidence is limited, but existing research demonstrates an upward trend in incidence within the U.S. and reveals disparities between sexes as well as racial and ethnic groups.1,3,4,5
The U.S. Lupus Midwest Network (LUMEN) has demonstrated several patterns in SLE, including increased prevalence, from 30.6 cases per 100,000 persons in 1985 to 97.4 in 2015, and a 2% increase in incidence each year, starting at 3.32 cases per 100,000 persons from 1976 to 1988 and ending at 6.44 from 2009 to 2018.1 The nation’s increasing racial and ethnic diversity, along with improved early detection of the disease, may contribute to this trend.1,6 LUMEN and other population-based studies have shown incidence rates three to seven times higher among women than men.3,4,7 Incidence rates were higher among non-Hispanic Black individuals of both sexes than among other groups.3,5
Compared to civilians, active component service members may have an increased risk of SLE due to greater exposure to environmental risk factors, such as silica dust and ultraviolet radiation, and higher rates of post-traumatic stress disorder, which have been linked to SLE.7,8,9,10 This study reports on annual incidence and sociodemographic disparities from 2000 to 2022 for ACSM in the U.S. Armed Forces diagnosed with SLE.
Methods
This study includes ACSM from January 1, 2000 through December 31, 2022, using data from the Defense Medical Surveillance System. Demographic variables of interest were sex, age, race and ethnicity, service, and rank. Diagnoses were ascertained from inpatient as well as outpatient encounter data of individuals who received medical care in the Military Health System or civilian facilities in the Click to closePurchased CareThe TRICARE Health Program is often referred to as purchased care. It is the services we “purchase” through the managed care support contracts.purchased care system.
SLE diagnosis was identified by International Classification of Diseases, 9th Revision code 710.0, or International Classification of Diseases, 10th Revision codes with all extenders under M32.11 An incident case was defined as one inpatient encounter with a qualifying code in the first or second diagnostic position, or the first of two outpatient encounters within 365 days at a rheumatology clinic (defined by Medical Expense and Performance Reporting code equal to “BAO”) with a qualifying code in any diagnostic position.11 The first encounter meeting the case definition with a qualifying code was considered the incident encounter. ACSM were counted only once during the surveillance period.
Incidence rates were calculated as SLE diagnoses per 100,000 person-years (p-years) using the mid-year population for each year of the surveillance period. Rates were stratified by age, sex, and race and ethnicity. Incidence rate ratios comparing non-Hispanic Blacks to non-Hispanic Whites, Hispanics, and other/unknown races and ethnicities were determined for each age group, stratified by sex.
Results
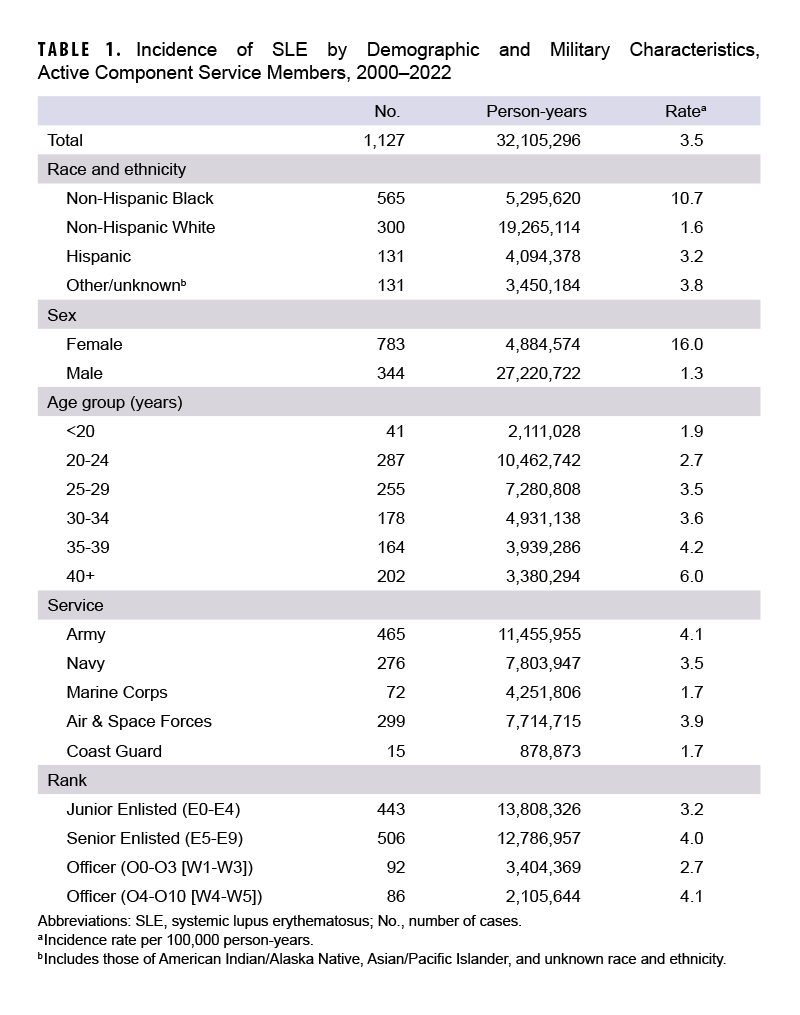
From 2000 to 2022, 1,127 ACSM were diagnosed with SLE. The number of incident cases was highest among ACSM aged 40 years or older, women, and non-Hispanic Black individuals (Table 1).
There were 545 (48.4%) ACSM incident SLE hospitalizations, with an average hospitalization of 4.7 days (standard deviation: 6.7, range: 0-60) (data not shown). Annual incidence for ACSM remained stable, ranging from 50 incident cases in 2000 to 44 in 2022 (data not shown). There was a slight increase in 2009, to 66 cases (data not shown).
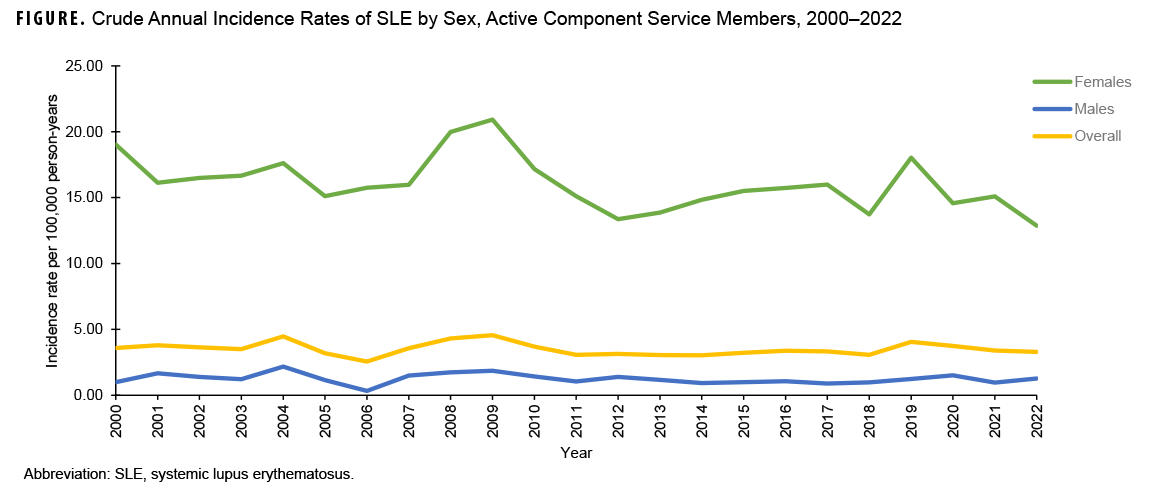
The overall incidence rate of SLE among ACSM from 2000 to 2022 was 3.5 per 100,000 p-years (Table 1). Service members aged 40 years and older had the highest rate of SLE compared to other age categories, with 6.0 cases per 100,000 p-years (Table 1). Non-Hispanic Black and female ACSM also had the highest incidence rates for their respective demographics, at 10.7 and 16.0 per 100,000 p-years, respectively (Table 1). Crude annual incidence rates among both sexes remained relatively constant throughout the surveillance period (Figure). Women started at 19.0 cases per 100,000 p-years in 2000 and ended at 12.9 in 2022, while men started at 1.0 case per 100,000 p-years in 2000 and ended at 1.3 in 2022 (Figure). Incidence rates for both sexes spiked during 2009, with women experiencing 20.9 cases per 100,000 p-years, while men experienced 1.9 cases per 100,000 p-years (Figure).
Incidence rates overall were highest among non-Hispanic Black ACSM and those of other/unknown race and ethnicity (Table 1). Non-Hispanic Black service members started at 10.1 cases per 100,000 p-years in 2000 and ended at 6.7 in 2022 (data not shown). Service members of other/unknown race and ethnicity started at 12.2 cases per 100,000 p-years in 2000, dropping to a low of 4.4 cases per 100,000 p-years in 2018, before increasing to 10.5 cases per 100,000 p-years in 2022 (data not shown). Meanwhile, non-Hispanic White service members began at 1.8 cases per 100,000 p-years in 2000 and ended at 2.4 in 2022, and Hispanic service members started at 2.5 cases per 100,000 p-years in 2000 and ended at 2.5 in 2022 (data not shown).
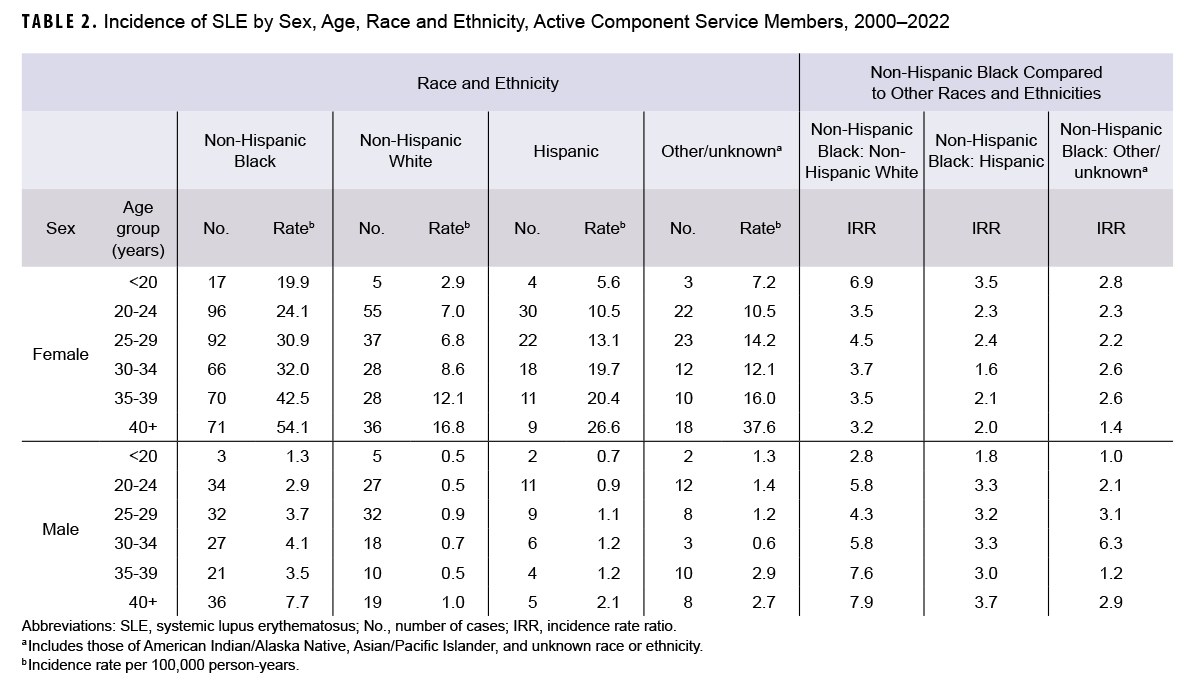
SLE incidence rates increased from 19.9 to 54.1 cases per 100,000 p-years for non-Hispanic Black women, compared to 2.9 to 16.8 for non-Hispanic White women with increasing age group (Table 2). Among all age groups and sexes, non-Hispanic Black ACSM had higher incidence rates of SLE compared to both their non-Hispanic White and Hispanic counterparts (Table 2). Incidence rate ratios comparing non-Hispanic Black to non-Hispanic White ACSM ranged from 2.8 to 7.9, while ratios comparing non-Hispanic Black to Hispanic ACSM ranged from 1.6 to 3.7, and ratios comparing non-Hispanic Black to the other/unknown racial and ethnic group ranged from 1.0 to 6.3 (Table 2).
Discussion
Overall, this study shows consistent SLE incidence rates among ACSM between 2000 and 2022, with the highest incidence among non-Hispanic Blacks and women. Existing research agrees with this disparity; other studies have shown significantly higher SLE incidence among non-Hispanic Black women.1,2,4,12,13 There is evidence suggesting those of African lineage are more likely than other races and ethnicities to possess a gene variant that increases SLE risk.14,15 There were more than twice as many incident cases among women (n=783) than men (n=344), and the overall incidence rate was 12.3 times higher among women. This trend was seen in rates for all ages as well as races and ethnicities, consistent with published statistics demonstrating that women are significantly more likely than men to develop SLE, perhaps due to differences in androgen levels and metabolism.4,12,13,16
Evidence shows that SLE is most common in women of child-bearing age (15 to 44 years). Women diagnosed with SLE aged 40 year or older may have developed the disease earlier in life but were not diagnosed until later.2,3,17 This is consistent with the findings of this study.
Unlike previous research of primarily civilian populations, this study found consistent incidence rates rather than increasing rates.1,3,4 This contrast may be due to better access to care for ACSM within the MHS, compared to other health systems that monitor civilians, allowing greater and earlier detection of SLE.
To our knowledge, this is the first study to show trends of SLE incidence in ACSM, yet there are limitations. This study relies on encounter data and does not use laboratory test data to confirm SLE diagnosis, which may have led to misclassification. For instance, patients may have been assigned SLE diagnostic codes based on physical examination and symptoms without laboratory tests confirming the diagnosis. Previous studies using similar case definitions displayed high sensitivity and specificity,11 but adding laboratory criteria to the case definition may be limiting, since the blood tests used to detect SLE are often positive in healthy individuals, leading to misdiagnosis.2 Likewise, this study did not use pharmacy data, such as the inclusion of selected medications including hydroxychloroquine, to confirm diagnosis.18 Future analyses may use pharmacy data to increase study specificity. Furthermore, race and ethnicity are self-reported; misclassification may occur due to limitations in how race and ethnicity are captured in DMSS. Despite these limitations, this study provides strong evidence that non-Hispanic Black women are disproportionately affected by SLE.
Although this disease is uncommon, its effects can be debilitating. ACSM who develop SLE may suffer from arthritis, pleuritis, and nephritis leading to kidney failure.19 These physical symptoms hinder ACSM abilities to execute military duties; 1 study demonstrated increased risk of discharge from the U.S. Army for service members with SLE.20 Analyzing trends in SLE incidence is valuable, to assess the burden and potential impact of SLE on mission readiness, for improved understanding and management of the disease among ACSM.
Authors' Affiliation
Defense Health Agency, Armed Forces Health Surveillance Division, Epidemiology and Analysis Section, Silver Spring, MD: Ms. Denagamage, Dr. Mabila, Ms. McQuistan.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the official policy of the Department of Defense nor the U.S. Government.
References
- Duarte-García A, Hocaoglu M, Valenzuela-Almada M, et al. Rising incidence and prevalence of systemic lupus erythematosus: a population-based study over four decades. Ann Rheum Dis. 2022;81:1260-1266. doi:10.1136/annrheum-dis-2022-222276
- Centers for Disease Control and Prevention. Systemic Lupus Erythematosus. Accessed Jul. 21, 2023. https://www.cdc.gov/lupus/facts/detailed.html#
- Duarte-Garcia A, Hocaoglu M, Osei-Onomah SA, et al. Population-based incidence and time to classification of systemic lupus erythematosus by three different classification criteria: a Lupus Midwest Network (LUMEN) study. Rheumatology (Oxford). 2021;61(6):2424-2431. doi:10.1093/rheumatology/keab807
- Izmirly PM, Ferucci ED, Somers EC, et al. Incidence rates of systemic lupus erythematosus in the USA: estimates from a meta-analysis of the Centers for Disease Control and Prevention national lupus registries. Lupus Sci Med. 2021;8(1):e000614. doi:10.1136/lupus-2021-000614
- Gianfrancesco MA, Dall'Era M, Murphy LB, et al. Mortality among minority populations with systemic lupus erythematosus, including Asian and Hispanic/Latino persons—California, 2007-2017. MMWR Morb Mortal Wkly Rep. 2021;70(7):236-239. doi:10.15585/mmwr.mm7007a2
- Uramoto KM, Michet CJ Jr, Thumboo J, et al. Trends in the incidence and mortality of systemic lupus erythematosus, 1950-1992. Arthritis Rheum. 1999;42(1):46-50. doi:w0.1002/1529-0131(199901)42:1<46::AID-ANR6>3.0.CO;2-2
- Bookwalter, DB, Roenfeldt, KA, Leard-Mann, CA et al. Posttraumatic stress disorder and risk of selected autoimmune diseases among US military personnel. BMC Psychiatry. 2020;20(1):23. doi:10.1186/s12888-020-2432-9
- Refai RH, Hussein MF, Abdou MH. et al. Environmental risk factors of systemic lupus erythematosus: a case-control study. Sci Rep. 2023;13(1):10219. doi:10.1038/s41598-023-36901-y
- Wolf ST, Kenney LE, Kenney WL. Ultra-violet radiation exposure, risk, and protection in military and outdoor athletes. Curr Sports Med Rep. 2020 Apr;19(4):137-141. doi:10.1249/JSR.0000000000000702
- Jones KA, Granado NS, Smith B, et al. A prospective study of lupus and rheumatoid arthritis in relation to deployment in support of Iraq and Afghanistan: the Millennium Cohort Study. Autoimmune Dis. 2011;2011:241267. doi:10.4061/2011/741267
- Moores KG, Sathe NA. A systematic review of validated methods for identifying systemic lupus erythematosus using administrative or claims data. Vaccine. 2013;31(Suppl 10):K62-K73. doi:10.1016/j.vaccine.2013.06.104
- Dall’Era M, Cisternas M, Snipes K, et al. The incidence and prevalence of systemic lupus erythematosus in San Francisco County, California: the California Lupus Surveillance Project. Arthritis Rheumatol. 2017;69(10):1996-2005. doi:10.1002/art.40191
- Izmirly PM, Wan I, Sahl S, et al. The incidence and prevalence of systemic lupus erythematosus in New York County (Manhattan), New York: the Manhattan Lupus Surveillance Project. Arthritis Rheumatol. 2017;69(10):2006-2017. doi:10.1002/art.40192
- Sibanda EN, Chase-Topping M, Pfavayi LT et al. Evidence of a distinct group of Black African patients with systemic lupus erythematosus. BMJ Glob Health. 2018;3(5)e000697. doi:10.1136/bmjgh-2017-000697
- Chae DH, Martz CD, Fuller-Rowell TE, et al. Racial discrimination, disease activity, and organ damage: the Black Women’s Experiences Living with Lupus (BeWELL) study. Am J Epidemiol. 2019;188(8):1434-1443. doi:10.1093/aje/kwz105
- Yacoub Wasef SZ. Gender differences in systemic lupus erythematosus. Gend Med. 2004;1(1):12-17. doi:10.1016/s1550-8579(04)80006-8
- Kernder A, Ritcher JG, Fischer-Betz R, et al. Delayed diagnosis adversely affects outcome in systemic lupus erythematosus: cross sectional analysis of the LuLa cohort. Lupus. 2021;30(3):431-438. doi:10.1177/0961203320983445
- Basta F, Fasola F, Triantafyllias K, Schwarting A. Systemic lupus erythematosus therapy: the old and the new. Rheumatol Ther. 2020;7(3):433-446. doi:10.1007/s40744-020-00212-9
- Shin JI, Lee KH, Park S, et al. Systemic lupus erythematosus and lung involvement: a comprehensive review. J Clin Med. 2022;11(22):6714. doi:10.3390/jcm11226714
- Nelson DA, Kaplan RM, Weisman MH, et al. Service discharges among US Army personnel with selected musculoskeletal and skin conditions: a retrospective cohort study. BMJ Open. 2022;12(10):e063371. doi:10.1136/bmjopen-2022-063371