This month’s edition of the MSMR Reportable Medical Events at Military Health System (MHS) facilities report provides an overview of annual data for 2025 for active component service members (ACSMs) and MHS beneficiaries. Reportable Medical Events (RMEs) are reported in the Disease Reporting System internet (DRSi) by health care providers and public health officials throughout the MHS for monitoring, controlling, and preventing the occurrence and spread of diseases of public health interest. These reports are validated by the Defense Health Agency–Public Health (DHA-PH).
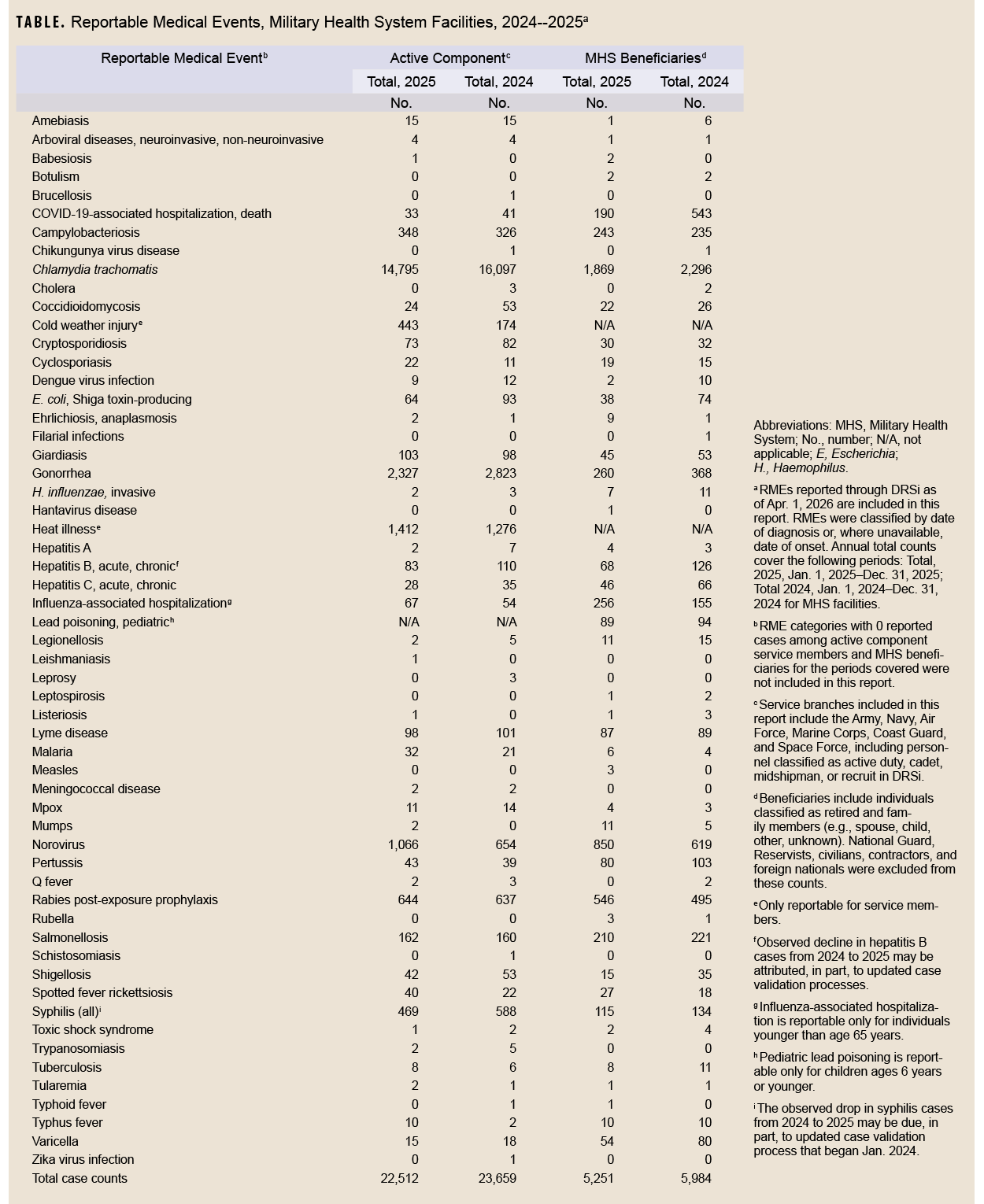
The DRSi collects reports on over 70 different RMEs, including infectious and non-infectious conditions, outbreak reports, sexually transmitted infection (STI) risk surveys, and tuberculosis contact investigation reports. A complete list of RMEs is available in the 2022 Armed Forces Reportable Medical Events Guidelines and Case Definitions.1 Data presented in this report are considered provisional and do not represent conclusive evidence until case reports are fully validated.
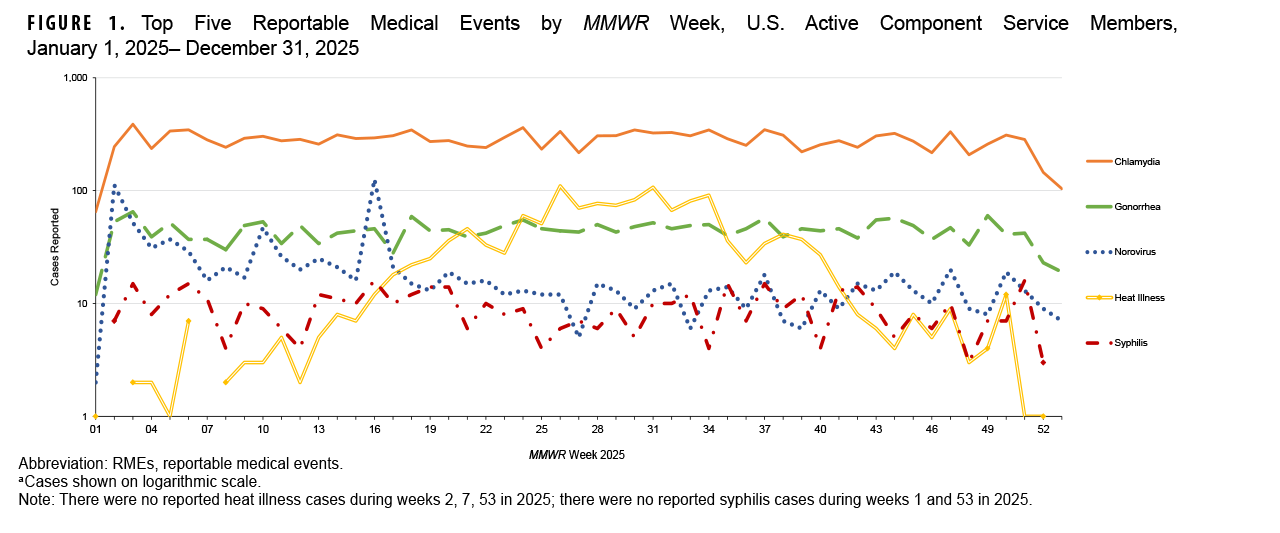
Top 5 RMEs in 2025, by MMWR Week, for ACSMs and MHS beneficiaries
The top 5 RMEs reported to DRSi in 2025 for ACSMs included chlamydia, gonorrhea, norovirus, heat illness, and syphilis (Figure 1), unchanged from 2024.
For MHS beneficiaries, the top 5 RMEs reported included chlamydia, norovirus, influenza-associated hospitalization, gonorrhea, and campylobacteriosis (Figure 2), similar to reporting in 2024, with the exception of influenza-associated hospitalization.

Ratios of RMEs for 2025 compared to 2024 for ACSMs and MHS beneficiaries
The current ratio data are based on incidence counts comparing year 2025 to 2024; low numbers for many conditions limit data interpretation and are not included in the figures. Conditions with less than 10 medical event reports (MERs) per year and syphilis were excluded from the ratio comparisons; syphilis and hepatitis B cases were excluded due to changes in case validation processes implemented throughout 2024. Ratios presented in Figure 3 and Figure 4 include any RMEs that had, at minimum, a 30% increase or decrease in MERs in 2025 respective to MERs in 2024.
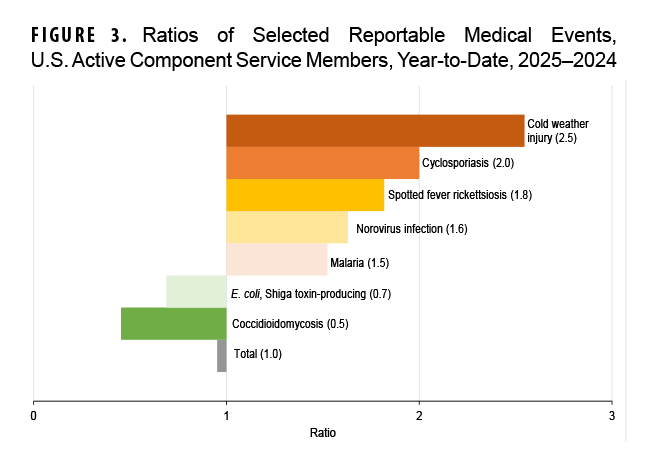
For ACSMs, the total number of MERs submitted to DRSi in 2025 decreased by 4.8% compared to 2024. Cases of cold weather injuries and cyclosporiasis had the most prominent increases in 2025 compared to 2024, with increases of 155% and 100%, respectively. Increases of case counts in 2025 were also recorded for spotted fever rickettsiosis (+82%), norovirus (+63%), and malaria (+52%). There were decreases in 2 RMEs in 2025 versus 2024 for ACSMs: for coccidioidomycosis (-55%) and E. coli, Shiga toxin-producing (-31%) (Figure 3).
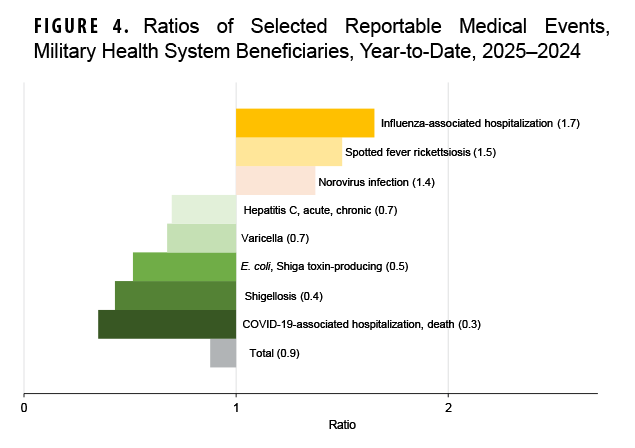
For MHS beneficiaries, the total number of MERs submitted to DRSi in 2025 decreased by 12.2% compared to 2024. MHS beneficiaries saw the most prominent increases for cases of influenza-associated hospitalizations and spotted fever rickettsiosis in 2025, with increases of 65% and 50%, respectively. Reports of norovirus also increased among MHS beneficiaries in 2025 versus 2024 (+37%). MHS beneficiaries saw the most significant decrease in cases of COVID-19-associated hospitalization and death (-65%) and shigellosis (-57%) compared to 2024. Decreases were also seen in reports E. coli, Shiga toxin-producing (-49%), varicella (-32%), and hepatitis C, acute and chronic (-30%) (Figure 4).
Discussion
Like the DHA-PH, the U.S. Centers for Disease Control and Prevention (CDC) reported similar trends for the increased influenza-associated hospitalizations in 2025 compared to 2024. The CDC classified the 2024-2025 influenza season as high severity, with the highest estimates of influenza-related illnesses and medical visits since the 2010-2011 influenza season.2 Hospitalization rates were equivalent in 2024-2025 to those during the 2017-2018 season, the last high-severity influenza season.2 Additionally, the CDC reported decreases in COVID-19 hospitalization rates from the 2023-2024 season to the 2024-2025 season, with a similar trend in the MHS.3
For questions about this report, please contact the Disease Epidemiology Branch at the Defense Centers for Public Health–Aberdeen. Email: dha.apg.pub-health-a.mbx.disease-epidemiologyprogram13@health.mil
References
- Armed Forces Health Surveillance Division. Armed Forces Reportable Medical Events. Defense Health Agency, U.S. Dept. of War. Accessed Apr. 1, 2026. https://health.mil/reference-center/publications/2022/11/01/armed-forces-reportable-medical-events-guidelines
- U.S. Centers for Disease Control and Prevention. 2024–2025 Influenza Season Summary: Severity, Disease Burden, and Burden Prevented. U.S. Dept. of Health and Human Services. Accessed Apr. 1, 2026. https://www.cdc.gov/flu-burden/php/data-vis-vac/2024-2025-prevented.html
- U.S. Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19) Hospitalization Surveillance Network (COVID-NET). U.S. Dept. of Health and Human Services. Accessed Apr. 2, 2026. https://www.cdc.gov/covid/php/covid-net/index.html